BIOLOGY 2F03 Lecture Notes - Lecture 7: Pulmonary Heart Disease, Tricuspid Insufficiency, Pulmonary Hypertension

19 May 2018
School
Department
Course
Professor

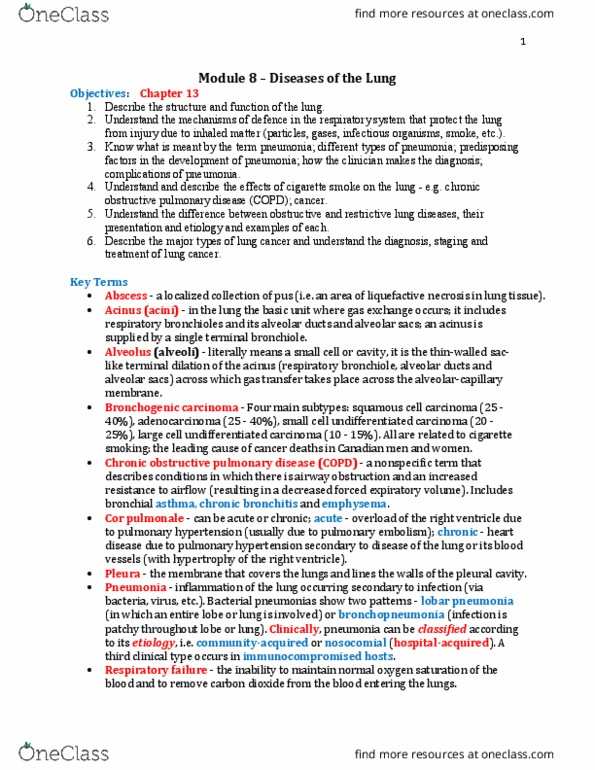
Pathology of the Lung
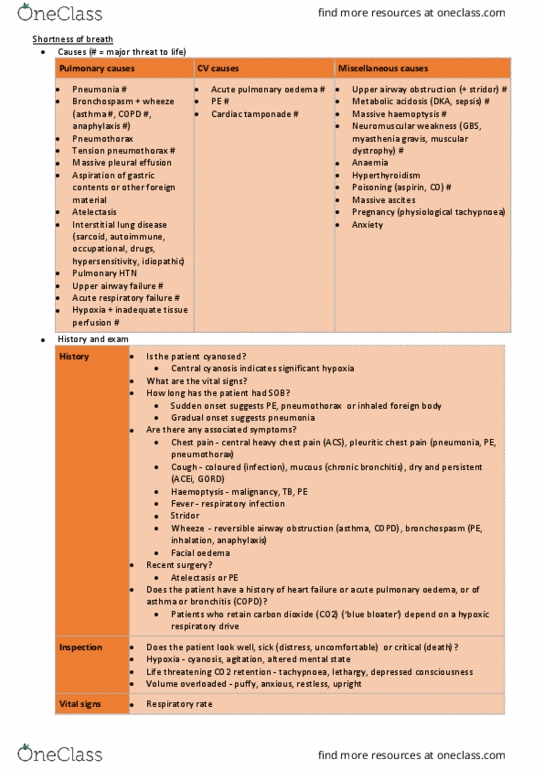
Respiratory Failure
• End-stage of all pulmonary disease
• PaO2 < 8 kpa
Type I respiratory failure
• Severe pneumonia, PE, asthma, fibrosis,
LVF
• V/Q Imbalance
o CO2 - Compensation (pCO2 -
normal/low)
o O2 – No compensation
Type II respiratory failure
• COPD, neuromuscular disease, severe
acute asthma
• Hypoventilation
o Impaired transfer of Co2 and O2
(pCO2 elevated)
Pulmonary Embolus
• 95% of PE from deep vein thrombi in legs/pelvis
• Large - Instant death (acute cor pulmonale)
• Medium - Chest pain + pulmonary heamorrhage
• Small - Cliically silet ultiple → Pul. HTN
• Ix: ECG + D-Dimer
Primary Pulmonary Hypertension
• Unknown cause
• > 25mmHg pressure at rest
• Young women
• Coplicatio → Right ventricular failure
• Tx: vasodilators/lung transplantation
RVF
• Causes:
o Left-sided heart failure
(congestive)
o Chroic lug pathology → cor
Pulmonale
• Consequences:
o Portal, systemic and peripheral
congestion
o Tricuspid regurgitation
o Renal congestion (R > L)
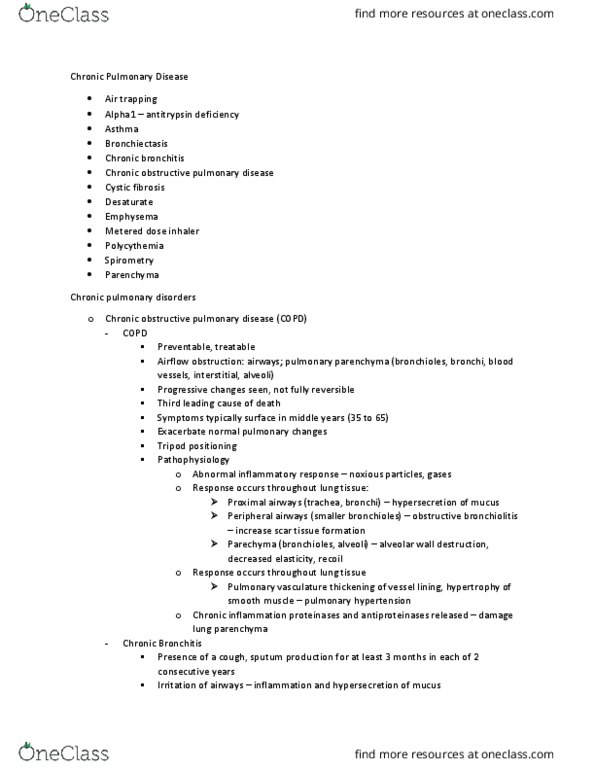
Obstructive pulmonary disease
These are characterized by an increased resistance to airflow (low FEV1 and FEV1/FVC < 0.7)
Asthma
• Kids > adults
• Chronic airways inflammation that is usually reversible
• Part of an atopic trait
• Can be severe and life-threatening
• Macroscopic
o Overinflated, patchy atelectasis, mucus plugs
• Microscopic
o Oedema, pulmonary infiltrates (eosinophils), smooth muscle and mucoal gland hypertrophy
Chronic bronchitis
• Chronic cough with production of sputum most days, for a least 3 months in 2 consecutive years
• Usually smoking/old patients
Emphysema
find more resources at oneclass.com
find more resources at oneclass.com