HTHSCI 1H06 Lecture Notes - Lecture 3: Truncus Arteriosus, Interatrial Septum, Brachiocephalic Artery

2 May 2018
School
Department
Course
Professor

Anatomy Midterm Review
THE CARDIOVASCULAR SYSTEM
Cardiac Development
- reason for development: a system is required to facilitate movement of materials
- 2 weeks: two tubes are present in the body of the embryo
- 4 weeks: the two tubes fuse
o the new single tube develops primitive sections called sacculations, with
narrowing between the five chambers
o chambers: truncus arteriosus bulbus cordis ventricle atrium
sinus venosus
o the tube is growing, becoming too long for the thorax, so it folds
▪ at this point, there is still a single tube: the atria are at the back,
ventricles are at the front, and the vessels exit cranially
▪ the valves form in the same plan along a diagonal line, dividing the
chambers (specifically between atria/ventricle and BC/TA)
- division of the truncus:
o an aorticopulmonary spiral septum grows inside the truncus, splitting it
into two, resulting in two separate vessels (aorta and pulmonary trunk) that
are spiraled around each other
▪ the heart also rotates, bringing the pulmonary trunk more to the left
▪ three veins emerge from the aorta (LR): subclavian,
brachiocephalic and common carotid
o two possible defects:
▪ 1) septum doesn’t spiral, great vessels are transposed
▪ 2) no septum forms, resulting in persistent truncus
▪ these would lead to mixing of oxygenated and deoxygenated
blood, and the baby would be cyanotic
- valve formation:
o as the growing septum results in the formation of the pulmonary trunk and
aorta, a semilunar tricuspid valve is formed for each (from one common 4-
cusped valve)
▪ pulmonary: anterior, left and right
▪ aortic: posterior, left and right
o as the division occurs, the left and right coronary arteries, which are fairly
posterior, become part of the aorta
o normal flow: blood is ejected from the ventricle and up either the
pulmonary trunk or aorta, after which the ventricle relaxes, causing
backflow of blood, resulting in the closing of the valve
- formation of the septa:
o interatrial septum: two septa are initially formed that contribute to its
development, the final septa is formed from both
find more resources at oneclass.com
find more resources at oneclass.com

▪ septum primum: develops first (at approximately 4 weeks), leaving
the foramen primum between it and the endocardial cushion. It
eventually fuses with the endocardial cushion
▪ foramen secundum (ovale): develops in the upper part of the
septum primum
▪ septum secundum: develops approximately 5 days later to the right
of the septum primum, covers the foramen ovale but does not fuse
to with the endocardial cushion to seal it
• need to leave a channel for shunting of blood from right to
left (pressure is greater on the right, pushing blood through
until the lungs start working)
• flow of blood reverses after the lungs begin to work
because pressure is reversed (greater on the left), the
foramen is closed, resulting in separate right and left
circulation
• patent foramen ovale: defect in foramen closure, gets worse
as you age and the right side of the heart has to work harder
and harder (it hypertrophies), shunt in the other direction
can eventually occur, resulting in bypassing of the lungs
(which are better equipped to deal with pathogens) directly
to the brain
o interventricular septum:
▪ a membranous part grows up to the endocardial cushion to divide
the ventricles into right and left
▪ malformation of the ventricular septum is the most common
congenital heart defect
• result: oxygenated blood flows directly from the left
ventricle into the right ventricle (after birth), where it mixes
with deoxygenated blood
• left ventricle hypertrophies
o vein formation: the superior and inferior vena cava arise from the sinus
venosus (the venous end of the heart tube)
- congenital heart defect summary:
o result: shunts (blood goes in the wrong direction) and obstructions (blood
can’t get to where it should go)
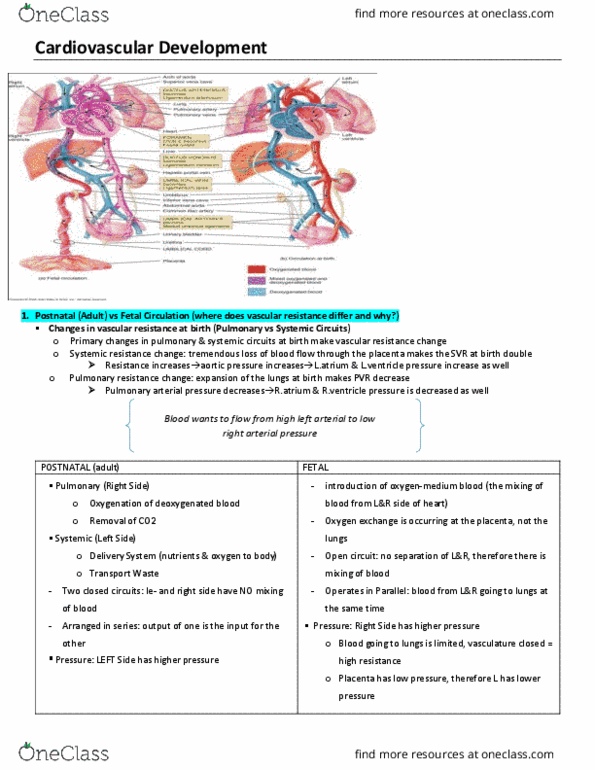
o flow is always high pressurelow pressure, right to left in the fetus, left
to right after birth (once the lungs begin working)
o examples: patent foramen ovale, atrial and ventricular septal defects
▪ Tetralogy of Fallot: Combination of pulmonary stenosis (very
narrow pulmonary trunk and valve), overriding aorta (thickens,
emerges from both ventricles), ventricular septal defect and right
ventricular hypertrophy (due to high pressure on the right side)
• Cyanosis occurs due to pumping of deoxygenated blood
into circulation and very little blood reaching the
pulmonary circulation
find more resources at oneclass.com
find more resources at oneclass.com

▪ Patent Ductus Arteriosus:
• The ductus arteriosus is a temporary shunt between the
aorta and the pulmonary trunk that normally closes shortly
after birth, forming the ligamentum arteriosum
• If it remains open, aortic blood flows into the pulmonary
trunk, increasing its pressure, resulting in overwork and
hypertrophy of both ventricles
▪ Coarctation of the aorta: a segment of the aorta is too narrow,
reducing the flow of oxygenated blood to the body, forcing the left
ventricle to pump harder, resulting in hypertrophy
• Can be above or below the ductus
• Sign: great upper limb pulses, but weak lower limb pulses
o they can present early or late, and are not always caught
▪ ventricular septal defect is picked up the most often, because you
can hear blood pressure much more regularly
o cyanosis: results from inadequately oxygenated blood
Cardiac Anatomy
- functions of the heart:
o pump blood to the lungs for oxygenation
o pump blood to the rest of the body for O2 transport, nutrient exchange, etc
- shape: resembles a closed fist (roughly the same size)
- location:
o lies in the mediastinum, two thirds to the left of the midline
▪ mediastinum: the mass of tissue that extends from the sternum to
the vertebral column between the lungs
o orientation is such that the apex (tip) of the heart points anterior, inferior
and to the left, while the broad upper base points posterior, superior and to
the right, some left ventricle is hidden posteriorly
▪ margins:
• anterior surface: deep to the sternum and ribs
• right border: faces the right lung, inferior surfacebase
• inferior surface: apexright border, rests on diaphragm
• left border: pulmonary border, baseapex, faces left lung
- important structures:
o pericardium: a tough fibrous sac surrounding the heart, confining it to the
mediastinum while still allowing space for contraction, slippery inside so
heart can move as it beats, several components:
▪ serous membrane: parietal layer covers the inner pericardial sac,
visceral layer covers the wall of the heart, they secrete the slippery
fluid so the two move in relation to each other
▪ layers (superficialdeep): fibrous pericardium parietal serous
pericardium parietal cavity visceral serous pericardium
(epicardium) myocardium (heart muscle, striated and
find more resources at oneclass.com
find more resources at oneclass.com
Document Summary
Cardiac development reason for development: a system is required to facilitate movement of materials. 2 weeks: two tubes are present in the body of the embryo. Pressures also measured at different points: to the end of ventricular repolarization: 1. Ventricular filling and atrial contraction (mid-late diastole: small elevation in ventricular pressure as they begin to fill, 2. Distribution of blood flow: 60% in veins and venules, 15% arteries and arterioles, 12% pulmonary vessels, 8% heart, 5% systemic capillaries. I, which goes through the lungs and is converted to angiotensin ii, which causes vasoconstriction and increased renal retention of salt and water, increasing arterial pressure. Blood composition in the average person: 55% plasma, 45% erythrocyte, <1% buffy coat (white blood cells/platelet, erythrocytes, white blood cells and platelts are the formed elements . Eosinophil, basophil or neutrophil: functional deficits: infection: increases the number of white blood cells, shift to left (neutrophils, eosinophils and basophils) leukemias: uncontrolled production and accumulation of immature leukocytes.