HTHSCI 2F03 Lecture Notes - Lecture 5: Brachial Artery, Cefotaxime, Reactive Arthritis

26 Dec 2020
School
Department
Course
Professor
Acute Osteomyelitis
Pathophysiology
Source: local or haematogenous.
Organisms
Staph
Strep
E. coli
Pseudomonas
Salmonella (in SCD)
RFs
Vascular disease
Trauma
SCD
Immunosuppression (e.g. DM)
Children
Rich blood supply to growth plate
usually affects metaphysis
Symptoms and Signs
Pain, tenderness, erythema, warmth, ↓ROM
Effusion in neighbouring joints
Signs of systemic infection
Investigations
↑ESR/CRP, ↑WCC
+ve blood cultures in 60%
X-ray:
Changes take 10-14d
Haziness + ↓ bone density
Sub-periosteal reaction
Sequestrum and involucrum
MRI is sensitive and specific
Management
IV Abx: Vanc + cefotaxime until MCS known
Drain abscess and remove sequestra
Analgesia
Septic Arthritis
Pathophysiology
Source: local or haematogenous.
Organisms
Staph: 60%
Streps
Gonococcus
Gm-ve bacilli
RFs
Joint disease (e.g. RA)
CRF
Immunosuppression (e.g. DM)
Prosthetic joints
Symptoms
Acutely inflamed tender, swollen joint.
↓ROM
Systemically unwell
Investigations
Joint aspiration for MCS
↑↑ WCC (e.g. >50,000/mm3) : mostly PMN
↑ESR/CRP, ↑WCC, Blood cultures
X-ray
Management
IV Abx: vanc + cefotaxime
Consider joint washout under GA
Splint joint
Physiotherapy after infection resolved
Complications
Osteomyelitis
Arthritis
Ankylosis: fusion
Differential
Crystal arthropathy
Reactive arthritis
© Alasdair Scott, 2012
124

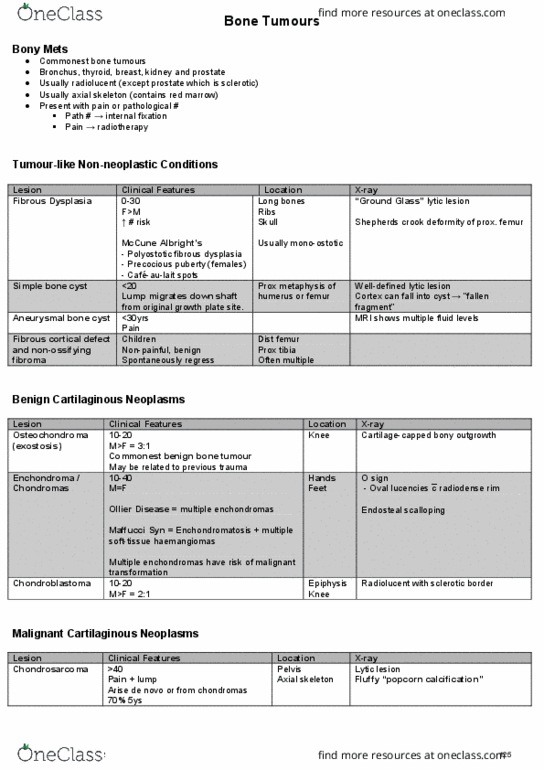
Bone Tumours
Bony Mets
Commonest bone tumours
Bronchus, thyroid, breast, kidney and prostate
Usually radiolucent (except prostate which is sclerotic)
Usually axial skeleton (contains red marrow)
Present with pain or pathological #
Path # → internal fixation
Pain → radiotherapy
Tumour-like Non-neoplastic Conditions
Lesion Clinical Features Location X-ray
Fibrous Dysplasia 0-30
F>M
↑ # risk
McCune Albright’s
- Polyostotic fibrous dysplasia
- Precocious puberty (females)
- Café-au-lait spots
Long bones
Ribs
Skull
Usually mono-ostotic
“Ground Glass” lytic lesion
Shepherds crook deformity of prox. femur
Simple bone cyst <20
Lump migrates down shaft
from original growth plate site.
Prox metaphysis of
humerus or femur
Well-defined lytic lesion
Cortex can fall into cyst → “fallen
fragment”
Aneurysmal bone cyst <30yrs
Pain
MRI shows multiple fluid levels
Fibrous cortical defect
and non-ossifying
fibroma
Children
Non-painful, benign
Spontaneously regress
Dist femur
Prox tibia
Often multiple
Benign Cartilaginous Neoplasms
Lesion Clinical Features Location X-ray
Osteochondroma
(exostosis)
10-20
M>F = 3:1
Commonest benign bone tumour
May be related to previous trauma
Knee Cartilage-capped bony outgrowth
Enchondroma /
Chondromas
10-40
M=F
Ollier Disease = multiple enchondromas
Maffucci Syn = Enchondromatosis + multiple
soft-tissue haemangiomas
Multiple enchondromas have risk of malignant
transformation
Hands
Feet
O sign
- Oval lucencies c
¯ radiodense rim
Endosteal scalloping
Chondroblastoma 10-20
M>F = 2:1
Epiphysis
Knee
Radiolucent with sclerotic border
Malignant Cartilaginous Neoplasms
Lesion Clinical Features Location X-ray
Chondrosarcoma >40
Pain + lump
Arise de novo or from chondromas
70% 5ys
Pelvis
Axial skeleton
Lytic lesion
Fluffy “popcorn calcification”
© Alasdair Scott, 2012
125

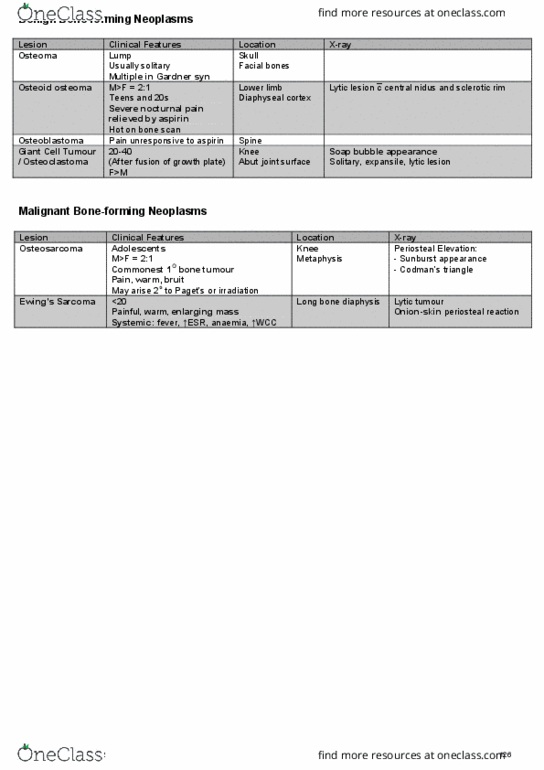
Benign Bone-forming Neoplasms
Lesion Clinical Features Location X-ray
Osteoma Lump
Usually solitary
Multiple in Gardner syn
Skull
Facial bones
Osteoid osteoma M>F = 2:1
Teens and 20s
Severe nocturnal pain
relieved by aspirin
Hot on bone scan
Lower limb
Diaphyseal cortex
Lytic lesion c
¯ central nidus and sclerotic rim
Osteoblastoma Pain unresponsive to aspirin Spine
Giant Cell Tumour
/ Osteoclastoma
20-40
(After fusion of growth plate)
F>M
Knee
Abut joint surface
Soap bubble appearance
Solitary, expansile, lytic lesion
Malignant Bone-forming Neoplasms
Lesion Clinical Features Location X-ray
Osteosarcoma Adolescents
M>F = 2:1
Commonest 1O bone tumour
Pain, warm, bruit
May arise 2o to Paget’s or irradiation
Knee
Metaphysis
Periosteal Elevation:
- Sunburst appearance
- Codman’s triangle
Ewing’s Sarcoma <20
Painful, warm, enlarging mass
Systemic: fever, ↑ESR, anaemia, ↑WCC
Long bone diaphysis
Lytic tumour
Onion-skin periosteal reaction
© Alasdair Scott, 2012
126
Document Summary
Iv abx: vanc + cefotaxime until mcs known. Wcc (e. g. >50,000/mm3) : mostly pmn. Cortex can fall into cyst fallen fragment . Usually radiolucent (except prostate which is sclerotic) Lump migrates down shaft from original growth plate site. Lytic lesion c central nidus and sclerotic rim. Roots leave vertebral column between scalenus anterior and medius. Divisions occur under the clavicle, medial to coracoid process. Plexus has intimate relationship c subclavian and brachial arteries. Median n. is formed anterior to brachial artery. Direct: e. g. shoulder girdle #, penetrating or iatrogenic injury. Leffert classification: open, closed, supraclavicular, infraclavicular, radiation-induced, obstetric, upper, lower, mixed. Loss of extension of cmc joints (finger drop) Site: # shaft of humerus where n. is in radial groove. Loss of sensation to dorsum of thumb root (snuff box) Site: axilla e. g. crutches or sat night palsy. Ulnar paradox: lesion at elbow has less clawing as. Fdp is paralysed, decreasing flexion of 4th/5th digits.