PAT 20A/B Lecture Notes - Anterior Interventricular Branch Of Left Coronary Artery, Posterior Interventricular Artery, Circumflex Branch Of Left Coronary Artery

2 May 2018
School
Department
Course
Professor

Winter Weeks 1 and 2: Coronary Artery Disease and Coronary Syndrome: Angina, Myocardial Infarction and Heart
Failure
Readings: Porth Chapters 24, 25, 26
Objectives:
1. Define and understand the classifications of angina.
2. Define and understand acute coronary syndrome (ACS), non–ST-segment elevation and ST-segment elevation
myocardial infarction (MI).
3. Comprehend the etiology, pathophysiology, manifestations, and complications of angina, ACS and MI.
4. Discuss the diagnosis and collaborative care of clients with angina, ACS and MI.
5. Identify the classifications of drugs used to treat angina, ACS and MI and state their mechanisms of action, desired
effects and adverse effects.
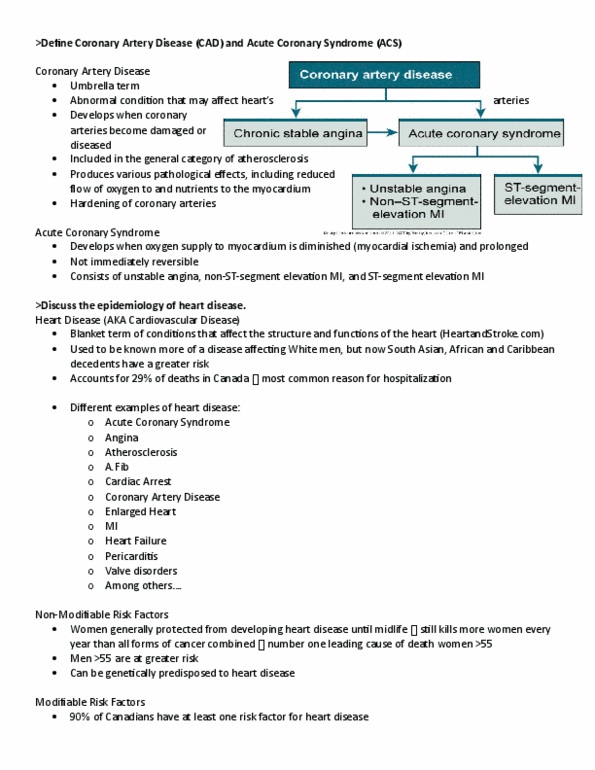
Coronary Artery Disease (Chapter 24)
• CAD: heart disease caused by impaired coronary blood flow; most cases caused by atherosclerosis
• Risk factors:
o Diabetes, smoking, HTN, elevated serum total & LDL cholesterol, low serum HDL, aging, abdominal obesity
and low physical activity
• Coronary Circulation: The Coronary Arteries (Know what parts of the heart they supply)
1. Left Main Coronary Artery
a. Left anterior descending = supply anterior wall of left ventricle
b. Circumflex branches = supply left lateral wall of left ventricle
2. Right Coronary Artery = supply right ventricle
a. Posterior descending artery (RCA moves to back of heart) = supply posterior heart, interventricular
septum, SA & AV nodes, posterior papillary muscle
Although RCA & LCA don’t connect there are anastomotic channels that join the small arteries;
o Gradual occlusion of the large vessels, smaller collateral vessels increase in size & provide
alternative channels for blood flow
o One reason CAD doesn’t produce symptoms until it is far advanced is that the collateral
channels develop at the same time the atherosclerotic chances are occurring
o Collateral Circulation: alternate circulation around a blocked artery/vein via another path
such as nearby minor vessels
• Control of Coronary Blood Flow: Physical, Neural, Metabolic
1. Physical
a. Coronary arteries originate from the heart = main factor responsible for perfusion of CA is the aortic
blood pressure
i. This aortic pressure moves blood through coronary vessels
b. Myocardial blood flow is regulated by the metabolic activity of the myocardium and auto regulatory
mechanisms that control dilation
c. Affected by systolic pressure that compresses the intramyocardial and subendocardial vessels
d. During contraction of the heart, there is compression, coronary arteries don’t get filled up at this time
2. Neural:
a. Exerts it’s effects on coronary blood flow through changes in heart rate, cardiac contractility & blood
pressure
3. Metabolic activity of the heart
a. Metabolites & endothelial mediators mediate vasodilation for increased blood flow & cardiac work
(adenosine)
b. Endothelial cells line blood vessels & CA form a selective barrier between the substances, molecules
& blood between intracascular and vascular tissue
c. Nitric oxide: vasodilator
i. Aggregating platelets, thrombin, increased shear force result in the synthesis & release of NO
= vasodilation
d. Endothelin: vasoconstricting factors
find more resources at oneclass.com
find more resources at oneclass.com

• Myocardial Oxygen Supply & Demand
o Myocardium: muscular tissue of the heart
o Coronary circulation supply’s heart muscle with O2 & nutrients to pump blood out to the rest of body; as
metabolic needs of the body changes = heart & coronary blood flow must adapt/adjust
o If there is an imbalance in myocardial oxygen supply & demand, myocardial ischemia/infarction sudden death
may occur
o Angina is associated with transient myocardial ischemia
o MI is associated with prolonged ischemia & cell death
o SUPPLY:
▪ Determined by CA and capillary inflow, and ability of Hgb to transport & deliver O2 to heart muscle
▪ Transport determined by the fraction of inspired oxygen in blood and number of RBC with normally
functioning Hgb
o DEMAND: 3 major determinants of MVO2
1. Heart rate
2. Contractility
3. Wall stress: tension is applied to an area
• Left Ventricular Wall Stress – is the average tension that muscle fibres must generate to shorten
against Intraventricular pressure
• At pressure: wall stress is increased by an increase in the radius (ventricular dilation) and increased by
a decrease in wall thickness
• REMINDERS:
o SYSTOLIC: amount of pressure in arteries during CONTRACTION
o DIASTOLIC: pressure when your heart muscle RESTS between beats
• PRELOAD: FILL / distending force of the ventricular wall; end of diastole; before contraction
o The volume of blood that fills the ventricles during diastole
o Influenced by the total volume of circulating blood
o The greater the venous return to the heart, the more the myocardial fibres will stretch to
accommodate that load
o Frank-Starling Law: the greater the myocardial fiber will stretch, the greater will be the force
of contraction
• AFTERLOAD: CONTRACT / load against which the heart must contract to eject blood; major
component is aortic pressure (pressure that the ventricle must generate to eject blood)
o The amount of tension the ventricles meet during systole (contraction)
o Some resistance is always present
o Increased afterload leads to: increased cardiac work and increased oxygen consumption
▪ if not meeting O2 demands = ischemia and infarction
• INCREASE in wall stress = INCREASE in MVO2
• Assessment of Coronary Blood Flow & Perfusion
1. Electrocardiogram (ECG): Diagnose & treat CAD, identify conduction defects, arrhythmias, electrolyte
imbalances, drug effects, electrical/structural abnormalities; Can see if there is MI (NSTEMI, STEMI)
2. Exercise Stress Test: observe cardiac function under stress; performed when ischemic heart disease symptoms are
present, checks physiologic response post MI or revascularization, post-op to assess factual status, evaluate
intermittent claudication; on treadmill = monitor BP & ECG & recorded to correspond with HR & potential
ischemic changes
3. ECHOcardiography: structure & function of heart, create moving image of internal structures of heart using
ultrasound signals that reflect when there is a change; determines ventricular dimensions, estimate diastolic &
systolic volumes
4. Nuclear Cardiac Imaging: gamma camera record the radiation emitted from radionuclide, PET uses positron-
emitting agents to demonstrate either the perfusion/metabolic status of the myocardium
5. Cardiac MRI & CT: MRI – spatially resolved map of radio signals; used for volume mass and function of
ventricles, cannot be used with persons with metal pacemakers, defibs, metal things / CT: x-ray based and obtain
cross sectional view of body, non-contrast CT: assess coronary artery calcification, contrast CT: assess cardiac
chambers/vessels/lumen; contraindicated for KIDNEY FAILURE PATIENTS: check creatinine levels
6. Cardiac Catheterization & Arteriography: catheters to view & record images of heart & vessels, measures pressure,
obtain samples for blood gas / angio: injecting radiographic contrast into heart to visualize moving structure
find more resources at oneclass.com
find more resources at oneclass.com

• Patho of CAD
o CAD = ACS + CIHD
▪ ACS: results from disruption of an atherosclerotic plaque that did not significantly compromise the
coronary lumen the event
▪ Unstable angina to MI (heart attack)
▪ CIHD: recurrent & transient episodes of myocardial ischemia and stable angina from narrowing of
CA
o Stable vs Unstable Plaque
▪ Stable: reduces blood flow distal to plaque – STABLE ANGINA
▪ Unstable: can rupture, cause platelet adhesion & thrombus formation – ACS
• Determinants of plaque vulnerability: large lipid core, thin fibrous cap, inflamm., lack smooth
muscle cells, located @ branch points or bends in arteries; diurnal variation (getting up in
morning)
o Thrombus & Vessel Occlusion
▪ Thrombus occurs after plaque rupture: exposure to substances from lipid core and provide stimulus for
platelet aggregation & thrombus formation
Acute Coronary Syndrome (pg 560): UA, NSTEMI, STEMI
• Physiological Changes in ACS
1. ECG Changes
• Classic changes:
o ST-elevation (transmural injury: entire wall thickness, epicardium) = when acute ischemia is
transmural, the overall ST vector is shifted in the direction of the outer epicardium, resulting in
ST elevation
o ST-depression (subendocardium): When ischemia is at the subendocardium, ST is shifted towards
innerventricular layer resulting in ST Depression
o T-wave inversion: First/earliest sign of ischemia
o loss of R-wave progression
▪ abnormal Q wave:
▪ wide and deep due to no depolarizing current in dead tissue, 1mm wide
• Repolarization phase of action potential is FIRST to be altered in myocardial ischemia & injury (T wave &
ST segment)
find more resources at oneclass.com
find more resources at oneclass.com
Document Summary
Winter weeks 1 and 2: coronary artery disease and coronary syndrome: angina, myocardial infarction and heart. Identify the classifications of drugs used to treat angina, acs and mi and state their mechanisms of action, desired effects and adverse effects. & blood between intracascular and vascular tissue: nitric oxide: vasodilator, aggregating platelets, thrombin, increased shear force result in the synthesis & release of no. Influenced by the total volume of circulating blood. The greater the venous return to the heart, the more the myocardial fibres will stretch to accommodate that load. Increased afterload leads to: increased cardiac work and increased oxygen consumption if not meeting o2 demands = ischemia and infarction. St segment: serum cardiac biomarkers, troponin (tni & tnt): calcium mediated actin-myosin contractile process in striated muscle. Primary & first biomarker; in cardiac muscle; Rise within 3 hours after onset of mi to 7-10 days after: creatine kinase mb (ck-mb): in muscle cells.