PSYB32H3 Lecture Notes - Lecture 10: Frontal Lobe, Parietal Lobe, Dual Diagnosis

23 Apr 2013
School
Department
Course
Professor
Document Summary
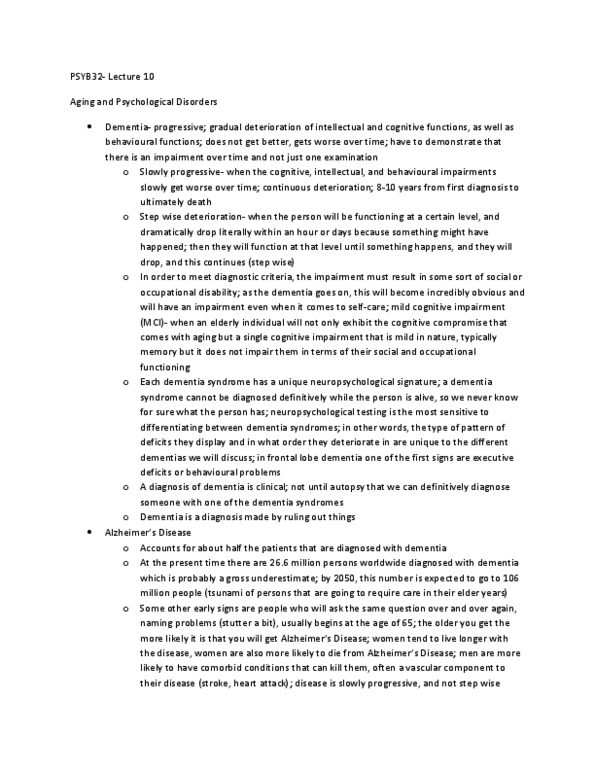
Neuropathology: brain with alzheimer"s = atrophy: wasting tissue/structure in certain areas (deeper creases), specifically the medial temporal lobes (language, hippocampus - memory formations) and parietal lobe (visual spatial deficit) and pre-frontal cortex (problem solving) Everyone has plaques and tangles in brain but the number of plaques and tangles is what differentiates. Literally count the number, certain number = alzheimer"s (can only be officially determined after autopsy) Dual diagnosis: dat post mortem, volume loss in hippocampus and temporal lobes (cortical level of brain outer layers) Sub-cortical levels remain intact (working memory, etc) ** Neuroimaging is helpful in the diagnosis of dat, but not a reliable marker. Neuropsychological tests of dat: neuropsychological signature of dat, memory, naming, visual spatial impairments profound deificits. Procedural memory relatively intact (habitual tasks: retrieval impaired, recognition impaired > remembering list of words (i. e. cvlt) Inability to spit out the word you want to say.