Kinesiology 3336A/B Lecture Notes - Lecture 17: Abductor Pollicis Longus Muscle, Scaphoid Fracture, Carpal Tunnel

18 Dec 2016
School
Department
Course
Professor
Document Summary
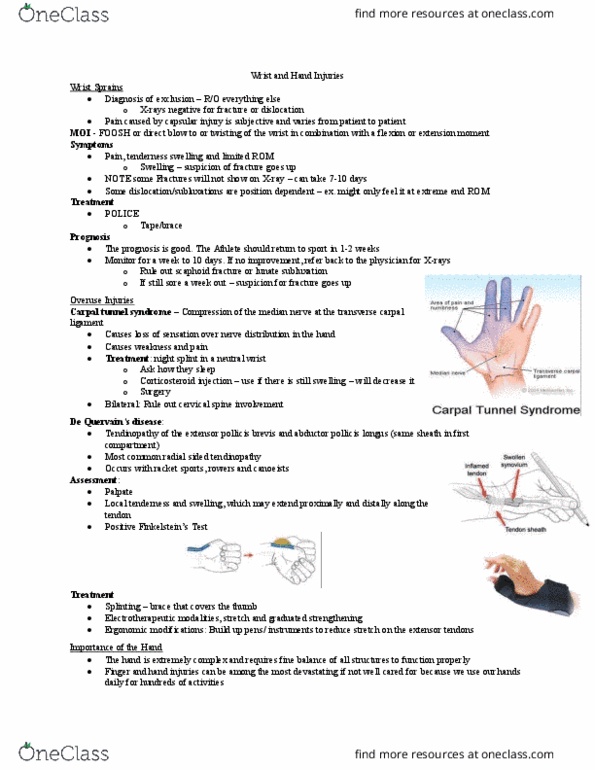
Diagnosis of exclusion: x-rays negative for fracture/ dislocation. Pain caused by capsular injury is subjective and varies from patient to patient. Twisting of the wrist in combination with a flexion/ extension movement. Note: some fractures wont show on x-ray. Prognosis= good: athletes should return to sport in 1-2 weeks. Monitor for 1 week- 10 days: if no improvement, refer back to physician for x-rays, may be a fracture not showing, take x-ray in a different position. Compression of the median nerve as it goes under the transverse carpal ligament. Causes loss of sensation over nerve distribution in the hand (gun fingers) Treatment: night splint in a neutral wrist: corticosteroid injection- decrease inflammation, surgery. Tendinopathy of the extensor pollicis brevis & abductor pollicis longus (go through same sheath in first compartment) Most common radial sided tendinopathy (really a tendinitis) Occurs with racquet sports, rowers and canoeists.