Physiology 3120 Lecture Notes - Lecture 4: Proximal Tubule, Epithelial Sodium Channel, Sglt2

9 May 2018
School
Department
Course
Professor

Physiology 3120
Dr. Woods
Lecture 4
Sodium Reabsorption
- Ion that drives reabsorption throughout the tubule bc the concentration is favorable along
majority of the way
- Na+ is very high outside of cells and very low inside of cells
- The outside of the tubule can be interstitial space, where the peritubular capillaries are or it can
be the filtrate, the inside of the tubule, the lumen, where the filtrate is
- The filtrate is derived from blood plasma
- Bc the filtrate is derived from blood plasma, plasma has a high concentration of Na+, which
filters into the tubule lumen so we have a great driver for ion movement and other solutes bc
Na+ pairs with a lot of other diff solutes to move into cells so we want this concentration
gradient from the filtrate into the tubule cells
- 30x concentration gradient from filtrate to tubule cells
- Na+ would like to move into tubule cells but requires transporters (channels/pore, carrier, etc)
- Examples:
o Sodium channels
▪ Simplest mechanism to move Na+ across the membrane
▪ Protein lined pore that recognizes Na+
▪ Ex: ENaC
• Family of channel
• Simple Na+ channel
• If there is a concentration gradient for Na+, Na+ can travel into or out of
the cell (in either direction)
• But generally, there is a favorable motion of Na+ into cells, so ENaC’s
allow Na+ to move from the filtrate into the tubule cells
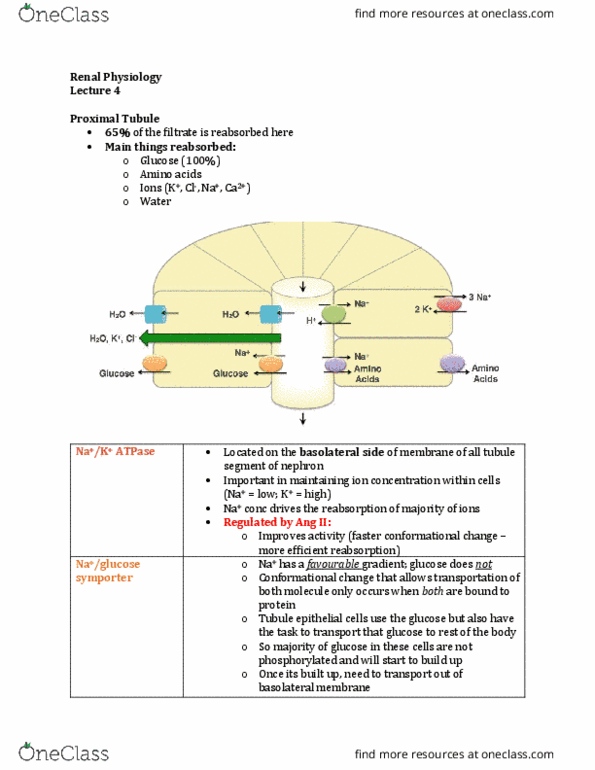
o Sodium symporters
▪ Protein carrier that binds to Na+ but also binds to other solutes within the
filtrate
▪ Ex: Na+/glucose symporters (SGLT1 & SGLT2)
• Protein carrier
• There needs to be physical binding of these items being transported
with the protein carrier embedded within the tubule cell membrane
• When both of the items are present (so we must have both these things
present and bound onto the protein carrier), the conformational change
occurs, the Na+ and the glucose move in the SAME direction INTO the
cell
• When you say Na+/glucose symporter, you are not just talking about 1
gene product, you are talking about multiple in the body
• There are 6 isoforms in the human body but SGLT1 and SGLT2 are the
most common in the kidney tubule
• SGLT1 and SGLT2 both move in one direction,
o but SGLT1 will move 2 Na+ ions for 1 glucose molecule
o while SGLT2 will move 1 Na+ ion for 1 Glucose
• SGLT2 is more highly expressed
▪ Protein carriers must still have a favorable concentration gradient – at least one
of the ions must have a concentration gradient so that the protein carrier can
change shape and move across the membrane
find more resources at oneclass.com
find more resources at oneclass.com

▪ Most of the time, Na+ is favorable and for ex here, glucose is non favorable
(going against its concentration gradient)
o Sodium exchangers
▪ Protein carrier that moves solutes in OPPOSITE directions across the membrane
▪ Ex: Na+/H+ exchangers (NHE3)
• Binds Na+ and binds H+ on opposite sides of the membrane
• Once both of those are bound, it exchanges the ions across the
membrane
• There are many isoforms of Na+/H+ exchangers, but in the kidney
tubule, NHE3 is the one that is highly expressed
• This exchanger is controlled by an important kidney hormone
o Sodium/Potassium ATPase
▪ Primary active transporters (use ATP directly) that use Na+
▪ Highly expressed in neurons, and most other cells
▪ Its an important protein carrier bc it maintains the ion concentration
differential – it keeps Na+ low inside of cells and K+ high inside of cells
▪ It moves Na+ and K+ across its gradient (which requires ATP) to maintain their
concentrations
▪ Expressed in EVERY epithelial tubule cell along the nephron
▪ But the position of the transporter is what makes it important – which
membrane it sits on will contribute to how well it works
Anion Transport – Chloride Reabsorption
- -ively charged ions have things that they need to overcome that the +ively charged ions dont
- Ion reabsorption must remain electroneutral
o This means we don’t want these cells to necessarily depolarize, we don’t want there to
be big shifts in voltage
o So when you are moving a -ive ion, you usually also move a +ive ion so that the inside of
the cell has the same charge
o This is true of all ions (we want to maintain electroneutrality with most of our
transporters)
- Chloride is the major anion reabsorbed
- Chloride Challenges:
o Transport is against an electrical gradient into tubule cells
▪ Cells of the body are more –ive on the inside than they are on the outside so in
order for Cl- to go into the cell, it is unfavorable electrically
▪ The inside of the cell has to change and become a little bit more +ive in order for
the Cl to even want to attempt to enter the cell
o Transport out of tubule cells must have a chemical gradient
▪ The outside of a cell is high in Na+ and Cl-
▪ So chemically, there is no favorable chemical gradient either for Cl-
▪ So for Cl- to get out of a tubule cell, into the interstitial space, Cl- has to
overcome a chemical gradient as well
- Examples of Cl- transporters:
o Chloride Channels
▪ If there is either a favorable chemical or electrical gradient, Cl- will move
through these channels
o Chloride symporters (ie. NCC)
▪ NCC = Na+/Cl co-transporter (co-transporter is the same as symporter)
▪ We use the Na+ concentration gradient and drag Cl- in the same direction,
against its either electrical or chemical gradient
o Chloride multiporters (ie. NKCC2)
find more resources at oneclass.com
find more resources at oneclass.com
Document Summary
Ion that drives reabsorption throughout the tubule bc the concentration is favorable along majority of the way. Na+ is very high outside of cells and very low inside of cells. The outside of the tubule can be interstitial space, where the peritubular capillaries are or it can be the filtrate, the inside of the tubule, the lumen, where the filtrate is. The filtrate is derived from blood plasma. Bc the filtrate is derived from blood plasma, plasma has a high concentration of na+, which filters into the tubule lumen so we have a great driver for ion movement and other solutes bc. Na+ pairs with a lot of other diff solutes to move into cells so we want this concentration gradient from the filtrate into the tubule cells. 30x concentration gradient from filtrate to tubule cells. Na+ would like to move into tubule cells but requires transporters (channels/pore, carrier, etc)