BIPN 100 Lecture Notes - Lecture 26: Macula Densa, Vascular Resistance, Arteriole

28 Jun 2018
School
Department
Course
Professor

BIPN100 Lecture 26 Notes 6/9/18
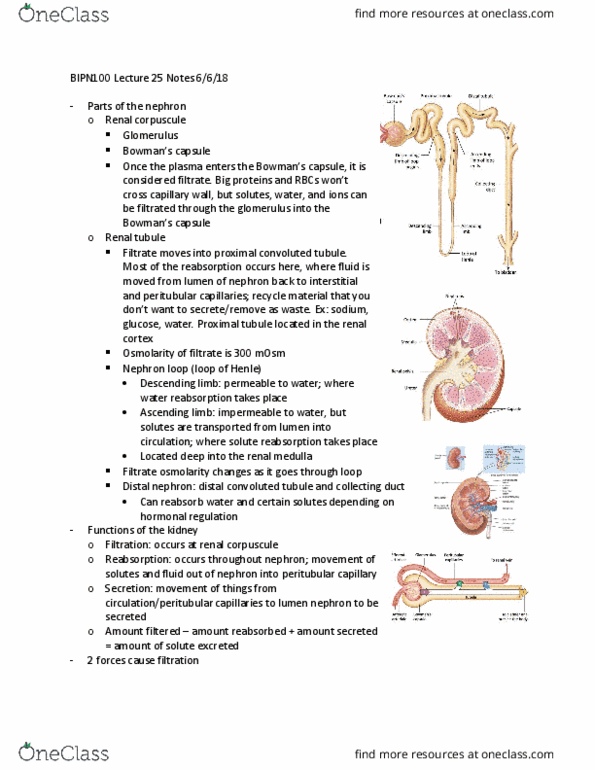
- Osmolarity changes through the
nephron
oDescending limb on loop of
Henle contains aquaporin 1.
There’s a driving force for water
to exit nephron, so water is
reabsorbed (from nephron to
interstitial fluid)
oNKCCs (Na+ K+ Cl- channels)
located on ascending limb of
loop of Henle. Due to Na+/K+
pump, there’s a driving force for
Na+ to enter, so Na+ enters, pulling 1K+ and 2Cl- in with it. Through leaked channels, the
ions exit the nephron and enter the interstitial fluid for reabsorption. Some ions are
reabsorbed, but some stay in the medulla to maintain the osmotic gradient
oEntering the distal tubule, fluid is hyposmotic at 100 mOsM. In distal tubule and
collecting duct, hormones can control reabsorption of water and solutes
If you’re dehydrated, want to recycle water. Collecting duct can contain aquaporins
on the apical membrane, under the influence of the posterior pituitary hormone
vasopressin (anti diuretic hormone, ADH)
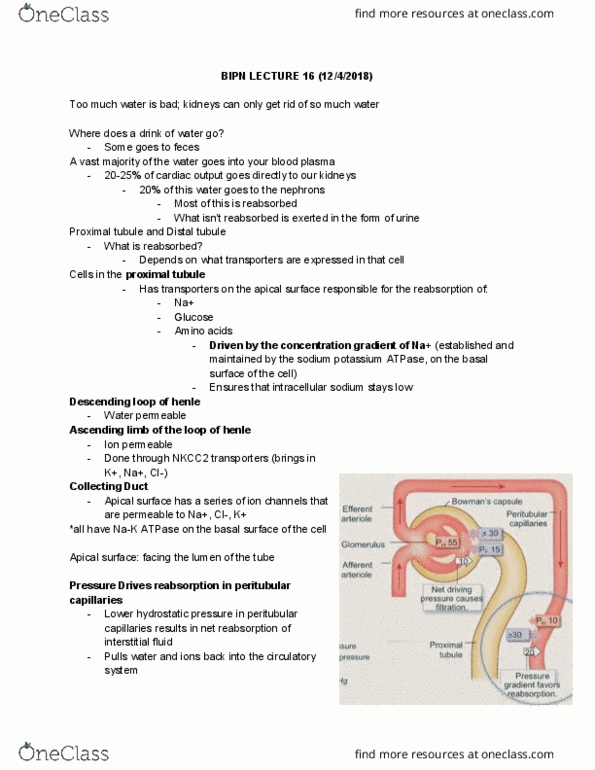
Membrane recycling: When you need to conserve
water, hypothalamus signals posterior pituitary
gland to release vasopressin into bloodstream.
Travels to collecting duct and binds to vasopressin
2 receptor (V2; membrane receptor) to activate Gs
transduction pathway. PKA phosphorylates
storage vesicles that contain aquaporin 2,
signaling them to fuse with apical membrane of
collecting duct. Now water can move through
pore from lumen -> cell -> interstitial fluid -> peritubular capillaries -> reabsorbed
When vasopressin is active, you have concentrated urine. When vasopressin isn’t
active, water isn’t reabsorbed in the collecting duct, so you have dilute urine
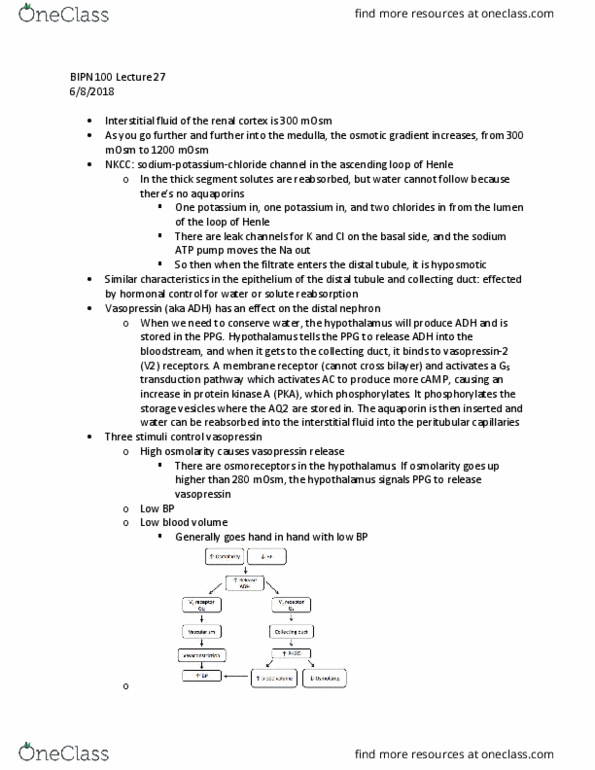
oControl of vasopressin (ADH)
Increased osmolarity and low blood pressure/low blood volume causes vasopressin
to be released
These stimuli activate 2 different pathways
In collecting duct, binds to V2 receptors to activate Gs pathway. This increases
water permeability, so water can be reabsorbed. This increases blood volume
(and blood pressure) and decreases osmolarity
find more resources at oneclass.com
find more resources at oneclass.com
Document Summary
Osmolarity changes through the nephron: descending limb on loop of. There"s a driving force for water to exit nephron, so water is reabsorbed (from nephron to interstitial fluid: nkccs (na+ k+ cl- channels) located on ascending limb of loop of henle. Due to na+/k+ pump, there"s a driving force for. Na+ to enter, so na+ enters, pulling 1k+ and 2cl- in with it. Through leaked channels, the ions exit the nephron and enter the interstitial fluid for reabsorption. Some ions are reabsorbed, but some stay in the medulla to maintain the osmotic gradient: entering the distal tubule, fluid is hyposmotic at 100 mosm. In distal tubule and collecting duct, hormones can control reabsorption of water and solutes. Collecting duct can contain aquaporins on the apical membrane, under the influence of the posterior pituitary hormone vasopressin (anti diuretic hormone, adh) Membrane recycling: when you need to conserve water, hypothalamus signals posterior pituitary gland to release vasopressin into bloodstream.