Case Study 1:
Medical History:
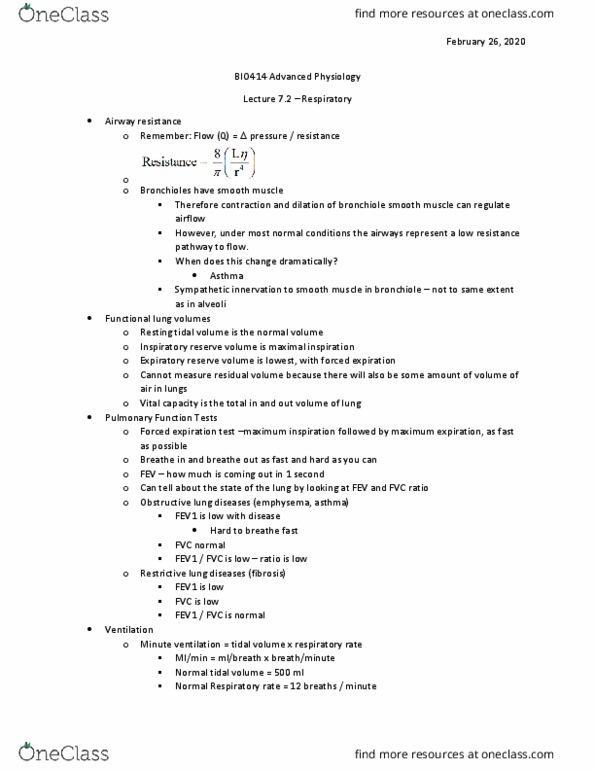
Ms. JR is a 22 yr old Caucasian college senior. Throughout high school she was active in competitive sports including soccer, swimming, and field hockey. On occasion throughout high school she would develop an increase in shortness of breath and a cough. Her primary care physician told her that she had bronchitis and that she should not worry about it. After entering college, she continued with competitive soccer and swimming. At the end of a long run during soccer games she would note an increase in cough and slight wheeze. She did not note any symptoms following her swimming practice. She continued to exercise but noticed an increase in coughing and wheezing over the ensuing year.
Diagnosis:
Her parents became concerned about her discomfort and tried to convince her not to exercise because âit makes you feel much worse and could be dangerous.â With ongoing symptoms, she withdrew from soccer. She sought advice of the college physician, who told her that she might have asthma given the symptoms of wheezing. Spirometry revealed an FEV1 of 3.09 L (96% predicted), an FVC of 3.54 L (95% predicted), a peak expiratory flow rate (PEFR) of 6.97 L (95% predicted), and an FEV1/FVC ratio of 87%. Given these results, showing ânormalâ pulmonary function, the patient was told that she did not have asthma but rather bronchitis and was advised to continue her exercise (after a course of antibiotics). She continued to swim but would note that at the end of a training session she was slightly more short of breath than usual and had anterior chest heaviness.
Exercise Test Results:
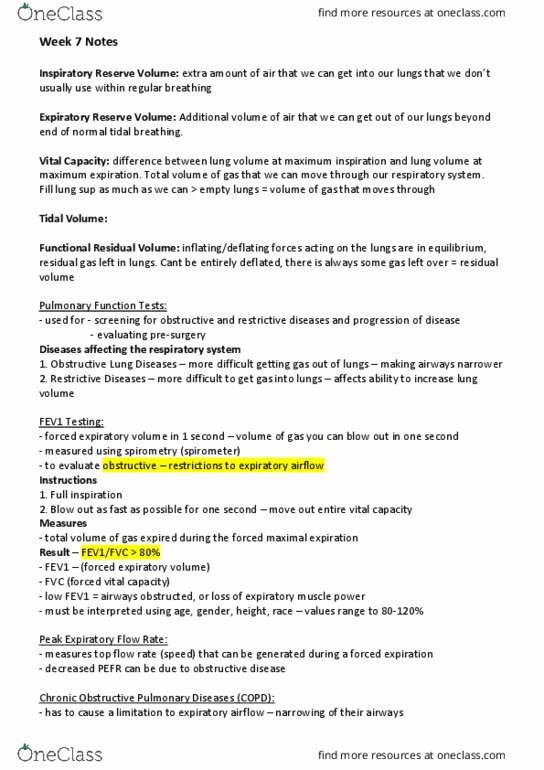
Ms. JR sought the advice of another physician, who ordered an exercise test with the measurement of expired gases during progressive incremental bike exercise. Spirometry was performed at 15, 30, and 60 min following the exercise test. Maximal oxygen consumption was 3.13 L · minâ1 (52.2 ml · kgâ1 · minâ1). Flow rates were as follows:
⢠FEV1 (L): preexercise = 3.09; 15 min postexercise = 2.87; 30 min postexercise = 2.20; 60 min postexercise = 2.24
⢠FVC (L): preexercise = 3.54; 15 min postexercise = 3.32; 30 min postexercise = 2.97; 60 min postexercise = 3.03
⢠PEFR (L/s): preexercise = 6.97; 15 min postexercise = 6.00; 30 min postexercise = 5.25; 60 min postexercise = 5.26
Exercise Prescription:
As a result of these studies, a diagnosis of asthma (exercise induced) was made. The patient was started on a short-acting b-agonist (albuterol sulfate) administered 30 min before exercise. She was instructed to warm up for 15 min with low- to moderate-intensity exercise or swimming before starting a high-intensity swim practice. Exercise tolerance subsequently improved while exercise-associated symptoms became rare (for the most part abated).
Questions:
1. Why was the initial diagnosis of asthma not entertained?
2. How was the actual diagnosis of asthma (exercise induced) made? What tests should be useful in this determination?
3. How did the recommendations improve the patientâs exercise tolerance? Why was swimming initially better tolerated than soccer?
4. Discuss the intensity, frequency, and duration of exercise training for patients with asthma.
5. How would the development of asthma symptoms at the end of a 3 h practice session influence the choice of medication (e.g., short-acting vs. long-acting b-agonist)?
Case Study 1:
Medical History:
Ms. JR is a 22 yr old Caucasian college senior. Throughout high school she was active in competitive sports including soccer, swimming, and field hockey. On occasion throughout high school she would develop an increase in shortness of breath and a cough. Her primary care physician told her that she had bronchitis and that she should not worry about it. After entering college, she continued with competitive soccer and swimming. At the end of a long run during soccer games she would note an increase in cough and slight wheeze. She did not note any symptoms following her swimming practice. She continued to exercise but noticed an increase in coughing and wheezing over the ensuing year.
Diagnosis:
Her parents became concerned about her discomfort and tried to convince her not to exercise because âit makes you feel much worse and could be dangerous.â With ongoing symptoms, she withdrew from soccer. She sought advice of the college physician, who told her that she might have asthma given the symptoms of wheezing. Spirometry revealed an FEV1 of 3.09 L (96% predicted), an FVC of 3.54 L (95% predicted), a peak expiratory flow rate (PEFR) of 6.97 L (95% predicted), and an FEV1/FVC ratio of 87%. Given these results, showing ânormalâ pulmonary function, the patient was told that she did not have asthma but rather bronchitis and was advised to continue her exercise (after a course of antibiotics). She continued to swim but would note that at the end of a training session she was slightly more short of breath than usual and had anterior chest heaviness.
Exercise Test Results:
Ms. JR sought the advice of another physician, who ordered an exercise test with the measurement of expired gases during progressive incremental bike exercise. Spirometry was performed at 15, 30, and 60 min following the exercise test. Maximal oxygen consumption was 3.13 L · minâ1 (52.2 ml · kgâ1 · minâ1). Flow rates were as follows:
⢠FEV1 (L): preexercise = 3.09; 15 min postexercise = 2.87; 30 min postexercise = 2.20; 60 min postexercise = 2.24
⢠FVC (L): preexercise = 3.54; 15 min postexercise = 3.32; 30 min postexercise = 2.97; 60 min postexercise = 3.03
⢠PEFR (L/s): preexercise = 6.97; 15 min postexercise = 6.00; 30 min postexercise = 5.25; 60 min postexercise = 5.26
Exercise Prescription:
As a result of these studies, a diagnosis of asthma (exercise induced) was made. The patient was started on a short-acting b-agonist (albuterol sulfate) administered 30 min before exercise. She was instructed to warm up for 15 min with low- to moderate-intensity exercise or swimming before starting a high-intensity swim practice. Exercise tolerance subsequently improved while exercise-associated symptoms became rare (for the most part abated).
Questions:
1. Why was the initial diagnosis of asthma not entertained?
2. How was the actual diagnosis of asthma (exercise induced) made? What tests should be useful in this determination?
3. How did the recommendations improve the patientâs exercise tolerance? Why was swimming initially better tolerated than soccer?
4. Discuss the intensity, frequency, and duration of exercise training for patients with asthma.
5. How would the development of asthma symptoms at the end of a 3 h practice session influence the choice of medication (e.g., short-acting vs. long-acting b-agonist)?