NUR1 420 Study Guide - Cirrhosis, Digoxin, Cardiac Output

7 Sep 2013
School
Department
Course
Professor
Document Summary
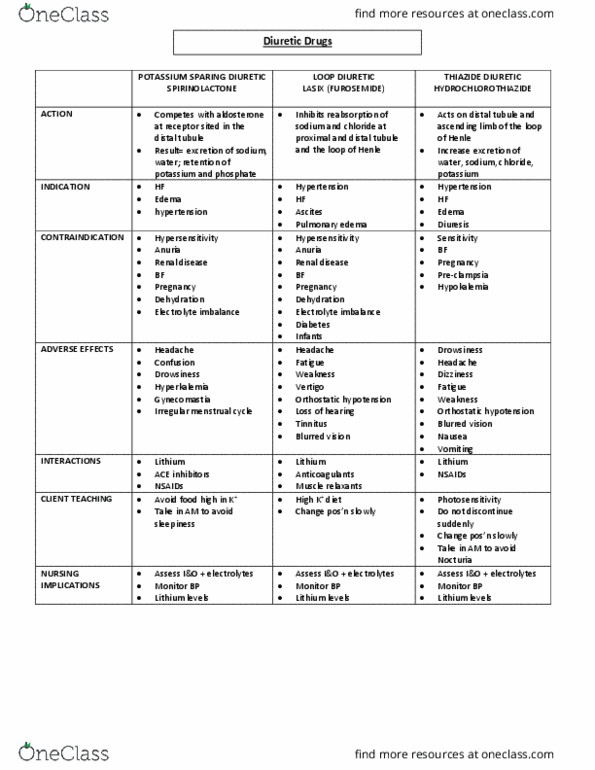
Interferes with absorption of sodium ions across the distal renal tubular segment of the nephron. This enhances excretion of sodium, chloride, potassium, bicarbonates, and water which decreases cardiac output and reduces plasma and extracellular fluid volume. Adjunct in treatment of edema associated with chf, hepatic cirrhosis, renal failure, and in the management of hypertension. Hypertension: adult: po 12. 5 100 mg/day in 1 2 divided doses. Edema: adult: po 25 200 mg/day in 1 3 divided doses. Mood changes, unusual tiredness or weakness, dizziness, light- headedness, paresthesia, irregular heartbeat, weak pulse, orthostatic hypotension, dry mouth, increased thirst, nausea, vomiting, anorexia, diarrhea, pancreatitis, jaundice, thrombocytopenia, hyperglycemia, and hypokalemia. Increased potassium and magnesium loss may cause digoxin toxicity. Increases risk of nsaid-induced renal failure and may attenuate diuresis. Hypersensitivity to thiazides or other sulfonamides; anuria; electrolyte imbalance. Antihypertensive effects may be noted in 3 4 days; maximal effects may require 3 4 wk.