PSYD35H3 Chapter Notes - Chapter 9, 10, 12-14: Μ-Opioid Receptor, Opioid Antagonist, Chemoreceptor Trigger Zone


Opioid Analgesics 3/5/2018 3:57:00 PM
PAIN TERMINOLOGY
• very common but difficult to measure because such a subjective
and personal experience
• “highly unpleasant sensory and emotional experience associated
with actual or potential tissue damage”
• acute, short acting, pain is biologically useful because it provides a
warning system against real or potential damage to the body
• chronic pain, however, serves no useful purpose, causes suffering,
limits activities of daily living
o lasts more than 3 months
o 2 types: nociceptive and neuropathic pain
o processes that increase or decrease nociception are
pronociceptive or antinociceptive (analgesic)
o nociceptive pain is caused by tissue damage … neuropathic
pain is caused by a lesion or some dysfunction of the NS
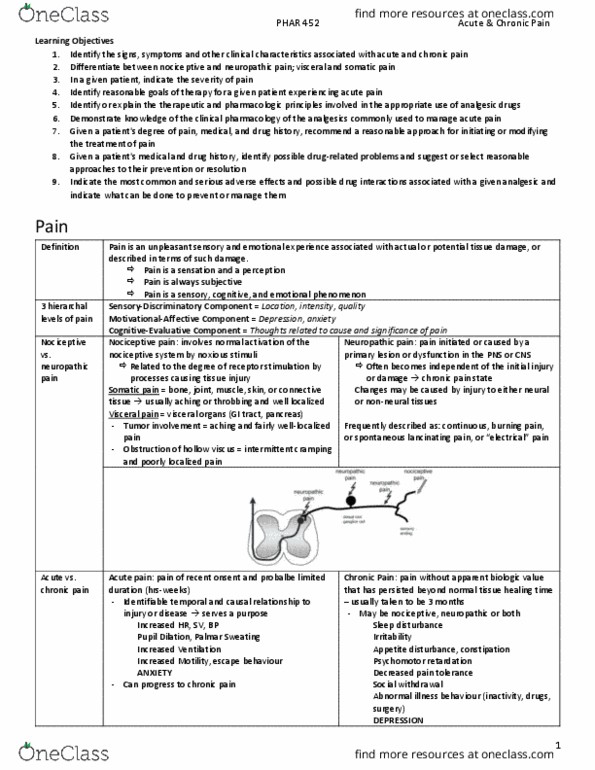
Pain Signaling
• noxious stimulus activates nociceptive primary afferents, whose cell
bodies are in the dorsal root ganglia (DRG) signals sent to dorsal
horn of spinal cord thalamus cortex and also other regions like
RVM (brainstem) and PAG (midbrain) inhibitory and excitatory
pathways descend from the brain back down to spinal cord and
modulate same PAG and RVM sites
• reduces inflammation
• blocks NMDA receptors in the spinal cord
OPIOID TERMINOLOGY
• opioid is any exogenous drug (natural, semisynthetic, or synthetic)
that binds to an opiate receptor, produces analgesia, and is blocked
by an opiate antagonist
• aka narcotic (sleep)
OPIOID RECEPTORS
• at least 3 types … all G-protein coupled receptors
• MOP, KOP and DOP
• each have own mRNA
find more resources at oneclass.com
find more resources at oneclass.com

• each is chain of 400 amino acids (60% identical and 40% different)
• possible subtypes
• all 3 distributed widely throughout CNS and lesser in PNS
o Mu found in high density except cerebral cortex
• miosis caused by action at kappa receptors
• endorphins exert most of their analgesic effects on descending
inhibitory neurons in the spinal cord
• activation of kappa causes dysphoria
• NOP does not respond to classical opiate antagonist, naloxone, so
debatable if actually an opioid receptor
• how does an opioid agonist interact with MOP’s?
o opioid binds activated G-protein, separating into alpha and
beta/gamma subunits activates K/ inhibits Ca/ reduces
cAMP hyperpolarization inhibition of neuron
• when activated, blocks release of pain-producing substances such
as glutamate substance P, and calcitonin gene-related peptide
(CGRP) reduces ascending pain signals to higher brain centers
• within the spinal cord, opiates inhibit pain primarily through axo-
axonic inhibition / presynaptic inhibition
CLASSIFICATION OF OPIOIDS
• laudanum = opium and ethanol
Pure Agonists
find more resources at oneclass.com
find more resources at oneclass.com

• all clinically used opioids produce their effects at least partly by
acting at the MOP receptor
• EX: morphine
Partial Agonists
• exerts an analgesic effect, but the effect has a ceiling at less than
the maximal effect produced by a pure agonist
• EX: buprenorphine … when given to opioid-dependent person it
competes with a full agonist withdrawal
Mixed Agonist-Antagonists
• produces an agonistic effect at one receptor and an antagonistic
effect at another
• lower efficacy than pure agonist
• like partial agonists, has ceiling effect for analgesia and lead to
withdrawal if given to opioid-dependent person
• EX: pentazocine
Pure Antagonists
• have affinity for a receptor, but after attaching they elicit no change
in cellular functioning (they lack intrinsic activity)
• compete with the mu agonist for the receptor, precipitating
withdrawal in an opioid-dependent person and reversing any
analgesia caused by the agonist
• causes decreased pain threshold and dysphoria
• EX: naltrexone
MAJOR PHARMACOLOGICAL EFFECTS OF OPIATES
Analgesia
• inability to feel pain or reduction to pain so it’s tolerable
• occurs without loss of consciousness and without affecting other
sensory modalities
• perception of the pain is significantly altered
Euphoria
find more resources at oneclass.com
find more resources at oneclass.com
Document Summary
Pain signaling: noxious stimulus activates nociceptive primary afferents, whose cell bodies are in the dorsal root ganglia (drg) signals sent to dorsal horn of spinal cord thalamus cortex and also other regions like. Rvm (brainstem) and pag (midbrain) inhibitory and excitatory pathways descend from the brain back down to spinal cord and modulate same pag and rvm sites: reduces inflammation, blocks nmda receptors in the spinal cord. Opioid terminology: opioid is any exogenous drug (natural, semisynthetic, or synthetic) that binds to an opiate receptor, produces analgesia, and is blocked by an opiate antagonist, aka narcotic (sleep) Classification of opioids laudanum = opium and ethanol. Pure agonists: all clinically used opioids produce their effects at least partly by acting at the mop receptor, ex: morphine. Analgesia inability to feel pain or reduction to pain so it"s tolerable: occurs without loss of consciousness and without affecting other sensory modalities, perception of the pain is significantly altered.