CAM201 Lecture 6: Pharmacology- Angina Notes

12 Jun 2018
School
Department
Course
Professor

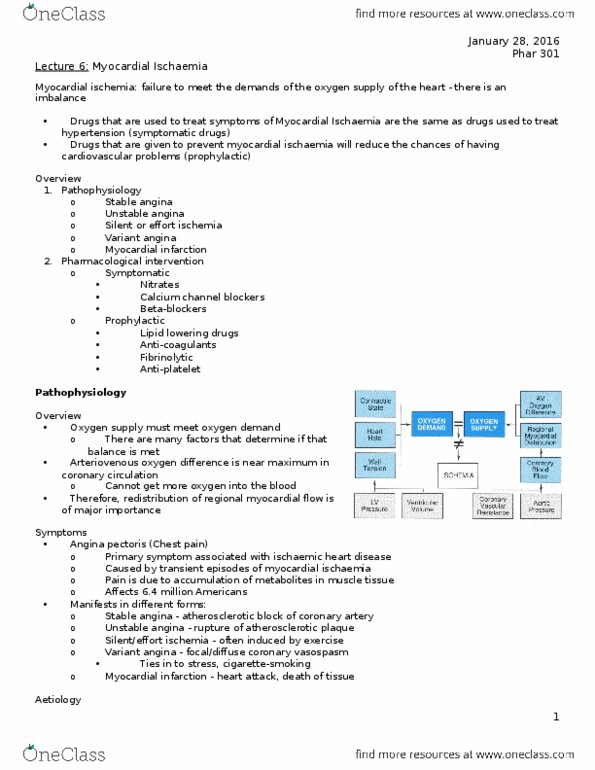
Angina
• Chest pain due to myocardial ischaemia (ischaemic heart disease)- insufficient
oxygen supply to myocardium- oxygen demands of the myocardium is not met
• Can be caused by coronary atherosclerosis (narrowing of vessel lumen) or
vascular spasm of the coronary vessels.
• The pain has a characteristic distribution in the chest, arm and neck.
• Pain may occur at rest, or may be brought on by exertion, cold or excitement.
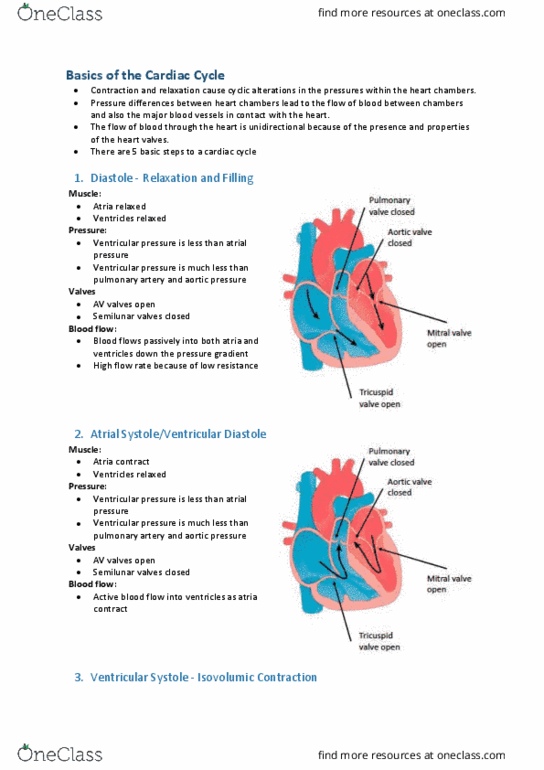
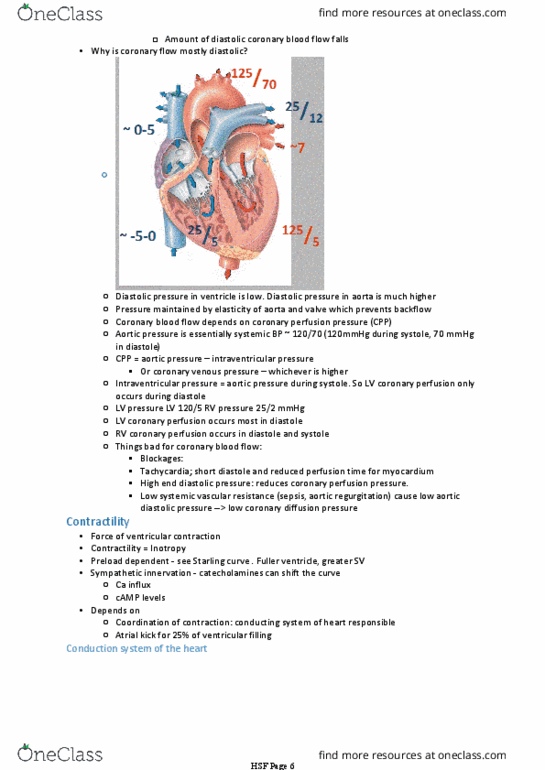
Factors Affecting Coronary Blood Flow
• The window for coronary blood flow is when aortic pressure is greater than coronary
blood flow.
• The window is during diastole
• The ‘window’ for coronary blood flow may be reduced by:
1. A shortened diastole (when the heart rate increases)- during exercise
2. Increased ventricular end-diastolic pressure- happens with stenosis of the aortic
valve, because more of the blood remains in the ventricles instead of being ejected
into the aorta through the valve
3. Reduced diastolic aortic pressure- also happens with stenosis of the aortic valve.
Types of Angina
Stable angina
• Predictable pain on exertion.
• Caused by a fixed narrowing of the coronary vessels, usually due to atherosclerosis.
find more resources at oneclass.com
find more resources at oneclass.com

Unstable angina
• A progressive form of angina – pain occurs more and more frequently and become
more severe over time.
• Pain starts off occurring with exertion only, but over time occurs during rest as well.
• Caused by thrombus associated with a ruptured atheromatous plaque (pathology similar
to myocardial infarction)
• Pharmacological management needs to be is aimed treating the underlying
atheromatous disease (e.g. high blood lipid levels) and not just improving perfusion.
• Risk of AMI is substantial, which can be reduced by aspirin
Classification of Coronary Ischaemia
• Non ST-elevation acute coronary syndrome (NSTEACS)
• Anti-platelet therapy is required to treat cute coronary syndrome to reduce the risk of
clotting- similar pathology of vessel damage → atherosclerotic plaque formation→
thrombosis formation → narrowing of vessel lumen
Coronary Artery Occlusion
• Atherosclerotic plaque can develop due to lipid accumulation in the vessel wall
• Plate aggregation can occur if the plaque becomes damaged due to high pressure, which
results in the formation of a thrombus
• Stable angina is due to a fixed obstruction (no platelet aggregation)
Pharmacological Management of Angina
• Drug therapy for angina is aimed at:
− Relaxing coronary artery smooth muscle (improving perfusion).
− Reducing the oxygen demand of the heart (decreasing cardiac workload).
• Short-acting organic nitrates are used for acute treatment
• Patients who suffer from frequent angina attacks can be prescribed drugs that can be
taken on a daily basis to reduce the frequency:
− Beta1 receptor agonists (cardio-selective beta blockers)- 1st line
− Calcium-channel blockers
Coronary
Ischaemic
Syndromes
Stable Angina
Acute
Coronary
Syndrome
STEMI NSTEACS
NSTEMI Unstable
Angina
find more resources at oneclass.com
find more resources at oneclass.com
Document Summary
Stable angina: predictable pain on exertion, caused by a fixed narrowing of the coronary vessels, usually due to atherosclerosis. Angina: non st-elevation acute coronary syndrome (nsteacs, anti-platelet therapy is required to treat cute coronary syndrome to reduce the risk of clotting- similar pathology of vessel damage atherosclerotic plaque formation thrombosis formation narrowing of vessel lumen. Pharmacological management of angina: drug therapy for angina is aimed at: Relaxing coronary artery smooth muscle (improving perfusion). Beta1 receptor agonists (cardio-selective beta blockers)- 1st line. Decreasing the opening of ca2+ channels- reduced contractility, less work. Activation of myosin light chain phosphatase (enzyme responsible for myosin light chain phosphorylation). Myosin light chain dephosphorylated- can no longer bind with actin, reduces heart contraction. Systemic effects: which vascular muscle the drug is targetting depends on dosage, therapeutic and adverse effects are dose related: At low doses, on cause venorelaxation with little effect on arterial resistance.