PHTY206 Lecture Notes - Lecture 14: Bursitis, Proprioception, Current History


Physical Examination of the Hip
• Learning Outcomes
o Describe the clinical presentation and pathology of common disorders of the hip
o List the various anatomical sources that may contribute to symptoms in the hip region
o Recognize clinical signs of a joint versus a muscle disorder in the hip
• **Note: revise functional anatomy of the hip and groin region
• Where is the pain coming from?
• Common Causes of hip pain
• Anterior Pain
o Hip Osteoarthritis (OA)
• OA is the soial joits age related respose to abnormal loading or abnormal
mechanics caused by a traumatic incident or repetitive microtrauma
• Trauma causes cartilage degradation, initiating an inflammatory process which
may lead to further cartilage damage.
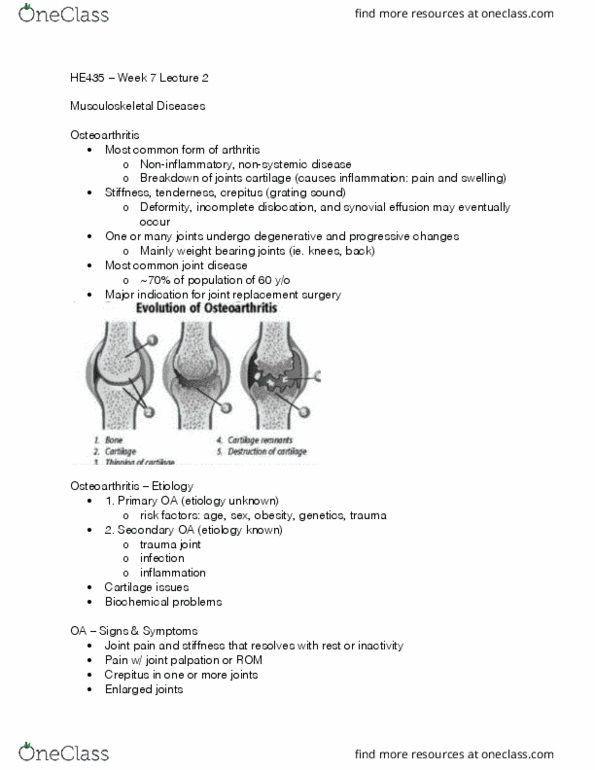
• OA can affect the whole joint organ (Brandt et al. 2009)
▪ Cartilage degradation
▪ Progressive damage to subchondral bone
• Microfractures
• Hypertrophic (osteophytic) and atrophic bone response
• Bone necrosis and periostitis
▪ Inflammation of the synovium and synovial lining thickening
• OA characteristics lead to pain & stiffness, to functional limitations and
subsequent muscle changes
• X-ray Diagnosis
▪ X-ray Diagnosis Kellgren & Lawrence scores 1-4
• Subchondral bone sclerosis
find more resources at oneclass.com
find more resources at oneclass.com

• Narrowing of joint space
• Formation of osteophytes at joint margin
• Subchondral cysts
• Superior migration of the femoral head secondary to articular
cartilage loss.
• Diagnostic Imaging for Hip OA
▪ Magnetic Resonance Imagining (MRI)
▪ Ultrasound
▪ Scintigraphy
▪ CT arthrography
• Used to identify early microscopic cartilaginous changes, bone marrow lesions
and oedema or other joint changes
• Hip OA vs. RA
OA
RA
• Local, usually affecting single joint,
develops gradually
• Morning stiffness < 1 hour
• Pain and stiffness in the affected joint
• X-rays - single hip joint usually affected,
subchondral bone sclerosis and osteocytes
• Autoimmune systemic disease, affecting multiple
joints with pain, stiffness and swelling (e.g. hands)
• Periodic flare up and remission
• Morning stiffness > 1 hour
• Fatigue, loss of appetite
• X-rays - may have bilateral hip joint signs,
demineralisation or femoral head, articular erosion
• Predisposing factors of OA
find more resources at oneclass.com
find more resources at oneclass.com

• Risk Factors
▪ Age - increased risk in >55yr olds, with further increased risk in 65 - 80 year
old
▪ Gender/sex - increased risk in women
▪ Genetic/familial predisposition
▪ Ethnicity or race - lower incidence in Asian cultures than white Caucasian.
Very low incidence in Koreans.
▪ Morphological abnormalities/developmental disorders
▪ Leg length difference
▪ History of lower limb or hip trauma
▪ Occupational factors
• Manual labour/physical stress work
• Sporting activities
▪ Increased weight or obesity (BMI) (questionable for development of OA but
yes for progression)
• American College of Rheumatology Clinical Diagnostic Criteria
• Patient Interview
▪ Main problem
• Joint pain & stiffness
• Pain usually related to movement e.g.: walking, driving, stair climbing,
gardening
• Stiffness in early morning or after rest which eases with movement
• Difficulty putting socks and shoes on
▪ Description of symptoms
• deep ahe or disofort ith sharp staig pai
• joint stiffness, restricted mobility
▪ Area of symptoms
• Reporting pain anterior/posterior or lateral hip region +/- referral to
thigh/knee
▪ Behaviour of symptoms
find more resources at oneclass.com
find more resources at oneclass.com
Document Summary
2009: cartilage degradation, progressive damage to subchondral bone, microfractures, hypertrophic (osteophytic) and atrophic bone response, bone necrosis and periostitis. Inflammation of the synovium and synovial lining thickening: (cid:1372) oa characteristics lead to pain & stiffness, to functional limitations and subsequent muscle changes, x-ray diagnosis, x-ray diagnosis kellgren & lawrence scores 1-4. Subchondral bone sclerosis: narrowing of joint space. Superior migration of the femoral head secondary to articular cartilage loss: diagnostic imaging for hip oa, magnetic resonance imagining (mri, ultrasound. Scintigraphy: ct arthrography, (cid:1372) used to identify early microscopic cartilaginous changes, bone marrow lesions and oedema or other joint changes, hip oa vs. ra. Leg length difference: morphological abnormalities/developmental disorders, history of lower limb or hip trauma, occupational factors, manual labour/physical stress work. Increased weight or obesity (bmi) (questionable for development of oa but yes for progression: american college of rheumatology clinical diagnostic criteria, patient interview, main problem.