PSYC 337 Lecture Notes - Lecture 9: Cortisol, Dsm-5, Anxiety Disorder

7 May 2018
School
Department
Course
Professor

Lecture 9: PTSD & OCD
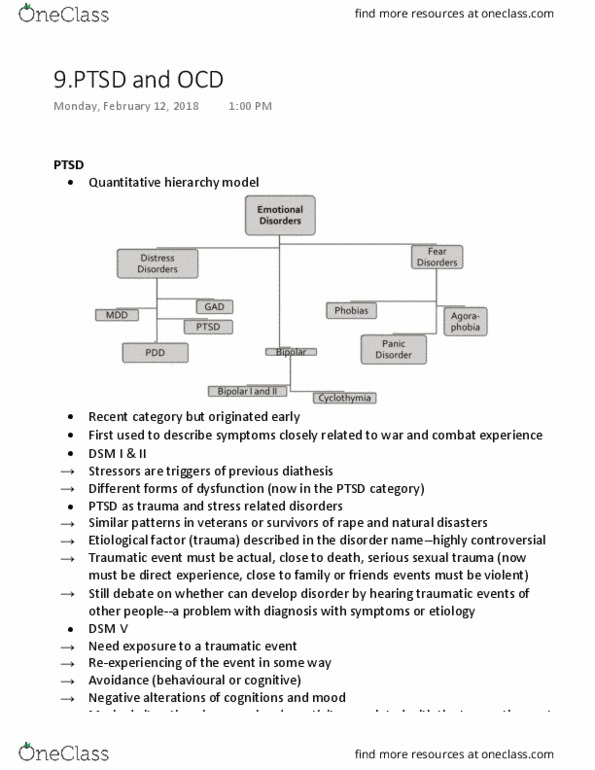
●Within the quantitative hierarchical model, PTSD fits in with the distress disorders
○Of note, it falls under the category of trauma-related
●PTSD
○Recent category, appearing first in DSM III
○But the roots go far back (especially with regards to soldiers coming back from war,
survivors of concentration or POW camps)
○In the DSM I and II, stressors were seen as triggers of pre-existing diathesis
■Forms of dysfunction that we now call PTSD were classified in other categories
according to the presenting symptomatology
■This changed a lot with the Vietnam War
●High rates of a disorder in soldiers, and other researchers were finding
similar patterns in survivors of rape and natural disasters
●This coalesced into a description of clinical picture now known as PTSD
○Departure from other DSM categories
■Trauma → is the presumed common etiological factor
●Disorder is organized around an etiological factor, unlike many other
disorders
●This is very controversial → should we include an etiological factor? Or
just describe symptoms
○DSM-5 criteria
■Need exposure to a traumatic event
●Actual or threatened death, or serious injury or sexual trauma
●Used to be that you could hear about an event happening to someone
you’re close to; now it has to be through direct experience, witnessing
firsthand, or learning about it affecting a loved one ONLY if it’s violent
■Need re-experiencing of the event in some way (e.g. dreams/nightmares,
flashbacks, constant intrusive thoughts)
■Avoidance (behavioural or cognitive)
■Negative alterations of cognitions and mood
■Marked alterations in arousal and reactivity associated with the traumatic event

●The research here is mixed in terms of hyperreactivity or blunting of
startle reflex
■Duration of disturbance is more than 1 month
○Epidemiology
■In DSM-III, thought to be rare (3%)
■Now, 7-8%
■2F:1M
■Rates of traumas are higher than the rate of PTSD
●60% of men and 51% of women report traumas that meet first criteria
●Why so many traumas but fewer PTSD cases?
○Among men, the most common trauma is violence (e.g. fighting,
robbery, etc.)
○Among women, the common would be sexual violence
○Possible that some traumas are more closely linked to
development of PTSD than others
●Overall, following trauma 9% develop PTSD
○Highest risk associated with assault or violence
■Kidnapped/torture (54%)
■Rape (50%)
■Cross-cultural
●Rates of PTSD are much higher in developing non-western countries
○Probably because many of these studies are done following
periods of turmoil and war
●Symptoms vary in different cultures
○E.g. after the Tsunami, the primary symptom was feeling
disconnected from your social roles/groups
○E.g. in Afghanistan, the primary symptom was a sense of internal
pressure in the body
■Predictors of PTSD following trauma
●Gender
○Even if people experience the same trauma, women are more
likely to be diagnosed with PTSD

●Familial psychopathology → nonspecific; just having a family member
with some form of psychopathology does predict greater vulnerability
●Preexisting psychopathology, especially depression
●Internalizing symptoms in early childhood
●Childhood or history of earlier traumas
●Lower IQ
●Nature of trauma
○Proximity → how close you were to the trauma (did it happen to
you, or someone else)
○Duration → being tortured for many years, versus several days
○Level of risk to life → if you believe you’re going to die during
the trauma
○Intention → if you believe the person who harmed you intended
to do so
○Psychological processes occurring during the trauma
○Dissociation → if you dissociate during the trauma (e.g. feel
you’re outside your body, can’t remember certain parts) it’s
more likely, and you’ll have a worse course/outcome
●Social support → this is protective, but people with PTSD can behave in
ways that decrease their social support
■Controversies in defining and classifying
●Most common → what constitutes a trauma?
●Is PTSD a normal response to an abnormal event, or an abnormal
response to a normal but stressful event?
○In DSM-III the event had to be outside the range of usual human
experience
○But, what events are outside the range of normal human
experience?
○Can PTSD result from normal events (e.g. car accidents)
○DSM-IV got rid of “normal human experience” concept
●Recent studies compared rates of PTSD following traumas and stressful
life events
Document Summary
Within the quantitative hierarchical model, ptsd fits in with the distress disorders. Of note, it falls under the category of trauma-related. Recent category, appearing first in dsm iii. But the roots go far back (especially with regards to soldiers coming back from war, survivors of concentration or pow camps) In the dsm i and ii, stressors were seen as triggers of pre-existing diathesis. Forms of dysfunction that we now call ptsd were classified in other categories according to the presenting symptomatology. This changed a lot with the vietnam war. High rates of a disorder in soldiers, and other researchers were finding similar patterns in survivors of rape and natural disasters. This coalesced into a description of clinical picture now known as ptsd. Trauma is the presumed common etiological factor. Disorder is organized around an etiological factor, unlike many other disorders. Actual or threatened death, or serious injury or sexual trauma.