MEDRADSC 2S03 Chapter Notes - Chapter 25: Etiology, Endoscopy, Trismus

25 Jun 2016
School
Department
Course
Professor
Document Summary
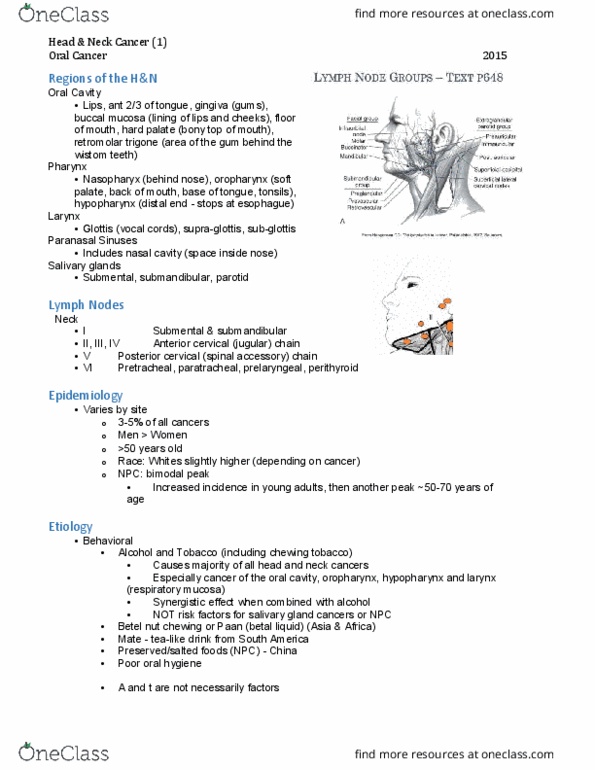
Upper part of pharynx behind nasal cavity. Bimodal peak; minor peak in young adults; major peak ~50-59 yrs, then decline in incidence in high risk areas. Tobacco has not been traditionally considered a risk factor for npc; however, outside of asia, where it is less common, tobacco is a risk factor. Starts in squamous cells lining the nasopharynx. Can spread into surrounding anatomy: ears, base of skull, eye sockets, invade nerves, lower pharynx, etc. Local recurrence is common due to local invasion before treatment. Typically spreads to cervical lymph nodes levels ii and iii; may then spread to level v; Often first spreads to ipsilateral side - progresses to bilateral involvement of neck nodes. Have distant metastases (25% cases have spread via blood) Often no s&s in early stage disease. Symptoms based on tissues invaded: hearing loss, tinnitus, nose bleeds/blockage o. Lump in neck most common late stage sign (ln)